Before delving into the problems of vitamin B complex deficiency and its symptoms, it is first important to understand the difference between vitamins that are in pill form versus vitamins that are contained within nature’s foods. There is a world of difference — a difference between sickness and health. Vitamins just do not work like foods, and foods are what our bodies were designed to use for healing, prevention and energy. There is no substitute, and no matter how you look at it, vitamin pills are an invention of scientists, so they are prone to cause side effects, be incomplete and lack what we need to overcome our health problems.
Vitamins have been sold and marketed as the “magic bullet” for all health problems, yet food science researchers are bringing out the truth about vitamins, minerals, multivitamins and antioxidants— and it’s not an easy pill to swallow. The problem is that vitamins, when not still contained in their original food (oranges, bananas, spinach, broccoli, etc.) are merely chemicals. Our bodies do not recognize vitamins as nutrients, because they don’t work the same way as whole foods for these simple reasons:
Foods contain not just vitamins, but the co-workers (synergists) and helper nutrients that allow vitamins to work
Foods are never found in high potency, so you won’t suffer any toxic side effects that have been proven to exist with ALL vitamin pills. As one expert stated, “Foods never deliver toxic doses [of vitamins]. (Hamilton, p.205)
Vitamins are just a small part of what our bodies require for health and healing. It is very often that it is the other food properties that help us while the vitamins are secondary.
Vitamin pills need other nutrients in order to work.
For these reasons, and more, vitamin pills, despite their use and overuse, are not turning people’s health around. They are lacking the properties of real nutrition which can only come from eating nature’s real, whole, raw foods. The only supplement that someone should take, therefore, is a whole food formula WITHOUT any isolated (singular vitamin). This is an important point, because most supplements called “whole food” are combinations of real foods and isolated vitamins. You have to carefully read the labels to see. Look for these words to identify vitamin chemicals on a label:
Pyridoxine
Thiamine or thiamin
Niacin or niacinamide
Palmitate
ascorbic acid
Riboflavin
Mixed tocopherols
B12
cyanocobalamin
more
Vitamins are not foods, so instead of vitamins and minerals on a label, you should be looking for the names of foods and herbs on the label. Don’t be fooled by high milligrams, high potency, standardization or any other such terms that just do not apply to real foods from nature.
VITAMIN B COMPLEX DEFICIENCY:
MAJOR CAUSES
Vitamin B complex comprises a number of vitamins that exist as a family. They should not be taken individually. In this modern era, millions of people suffer from a deficiency of vitamin B for several reasons, chief among which are:
Stress: emotional, physical and spiritual
Processed foods in the diet: these are not real foods and so they tax the body
Refined sugar. The average person consumes at least 140 pounds of sugar a year which robs the body of its vitamin B stores
Drugs: both recreational and prescription drugs deplete vitamin B
Toxins: poisons in the environment and personal care products deplete vitamin B complex
Malnutrition. Most people are malnourished because they are not eating the right kinds of foods
Cooking. Most people do not eat enough real, raw foods, so vitamin B is killed or so depleted that people are not getting enough of it in the diet
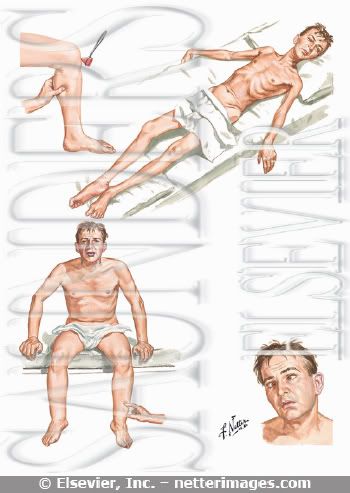
DO YOU HAVE ANY OF THESE SYMPTOMS?
Once your body has been deprived of the vitamin B complex due to reasons stated above, it begins to show symptoms (signs) of altered, diminished or poor health. This is because the vitamin B complex (within foods, not vitamin pills) is responsible for such a wide variety of activities, including cellular differentiation, transmission of nerve electricity, health of nerve cells, heart pulse rate, muscular contraction, digestion, brain function, thought processes and energy production. Without adequate vitamin B complex from foods, you can experience one or more of any one of these symptoms:
mental problems
heart palpitations
heart arrythmias
fibrillation
indigestion
chronic fatigue
chronic exhaustion
paranoia, vague fears, fear that something dreadful is about to happen
nervousness
ADD (attention deficiency), inability to concentrate, irritability
feeling of uneasiness
thoughts of dying
easy agitation, frustration
inability to sleep (insomnia)
restlessness
tingling in hands
tingling fingers and toes
rashes
crying spells, inability to cope
soreness all over
and so much more.
CHRONIC VITAMIN B DEFICIENCY
Vitamin B deficiency can sneak up on you, because it doesn’t have to create serious health problems right away. In fact, medical researchers have discovered that very often there can be no detectable signs according to scientific instrumentation, that you are experiencing a deficiency. For example, “memory impairment due to vitamin B12 deficiency can precede blood symptoms of deficiency by years. Evidence that vitamin B12 deficiency accounts for some cognition deficits in older people comes from a study that revealed abnormal short-term memory in more than two-thirds of clients with pernicious anemia…The researchers recommend that a diagnosis of senile dementia should not be made, even in the absence of anemia, until vitamin B12 status is determined biochemically.” (Hamilton, p. 476) This means that it is possible that certain mental disorders can be directly attributable to vitamin B complex deficiency, and it is easier to first start replenishing stores of vitamin B complex than to begin treating difficult mental illnesses with drugs, therapy or psychological counseling.
When vitamin B deficiency becomes chronic (long-lasting), other problems can occur, including troubles with your adrenal system. The adrenal glands serve many purposes, but in relation to this topic, they are the back up system for making energy. When there is a chronic lack of vitamin B complex then the adrenal glands are called upon to produce quick energy by injecting certain hormones like adrenaline into your system so that you can cope with life. If this goes on for a long time, then the adrenal glands become impaired or worn out, leading to even more health problems.
WHAT YOU CAN DO TO HELP YOURSELF
There are a number of things you can do to prevent and overcome vitamin B complex deficiency:
1. Stop taking vitamin pills and switch over to
NutriPlex Whole Food Formulas products. The three most recommended to support you are: BFood Complex, AdrenaPlex and SuperGreens PhytoFood. These products are made only of foods and not parts of foods or isolated vitamins. They won’t add to your problems the way vitamin pills can, and they are not toxic the way vitamin pills can be.
2. Stop eating refined sugar.
Click here to read all about refined sugar and its bad effects from researcher Nancy Appleton, PhD.
3. Stop eating artificial ingredients. Read all labels on your foods and if there are names of chemicals, don’t eat them. (Read the author’s book, Illness Isn’t Caused by a Drug Deficiency. Switch to
organic foods.
4. Reduce stress through a regular exercise program, meditation, counseling and/or hobbies
5. Stop drinking coffee; switch to organic decaffeinated coffee or organic green tea
6. Eat more vitamin B-containing foods — oats, barley, wheat bran, avocado, salmon, Brazil nuts and others.
7. Be patient. It took a while to create a vitamin B deficiency, so it takes a while to reverse the problem; with severe cases it can take a year or so, with milder cases it can take just a few days.
8. If you have a friend or relative with a mental or emotional disorder, think of the possibility of a vitamin B complex deficiency and then make suggestions for adjustments in their diet and take appropriate whole food formulas.
9. Always coordinate all of your health and treatment plans with all of your practitioners.
10. Avoid toxins in your life. This is a serious issue that causes more health problems than people commonly realize. (See the author’s book, Evil Genius in the Garden of Eden — how toxins make us sick and corporations profit from our illness).
Sources:
Journal of the American Medical Association (JAMA); “Vitamins for Chronic Disease Prevention in Adults,” Clinical Applications, Robert H. Fletcher, MD,MSc; Kathleen M. Fairfield, MD,DrPH
JAMA. 2002;287:3127-3129.
Shayne, PhD, Vic, Man Cannot Live on Vitamins Alone, 2004
Shayne, PhD, Vic, Illness Isn’t Caused by a Drug Deficiency!, 2001
Hamilton, et.al, Nutrition Concepts & Controversies, 5th Ed., West Publishing, St. Paul, 1991
Stryer, PhD. Lubert, Biochemistry, 2nd Ed., Stanford University, WH Freeman & Co., San Francisco, 1981
About the AuthorDr. Vic Shayne is a doctor-consultant and food science researcher and author whose website is
www.nutritionresearchcenter.org. ©2005 Dr. Vic Shayne. This article may not be used in conjunction with the promotion or sale of any product unless authorized in writing by the author.